May 22, 2026
Hantavirus Outbreak: Understanding Transmission and Public Health Preparedness

Epidemiology & Public Health Risk
Zoonotic Pathogen I Rodent- Borne Transmission I No Approved Treatment
Authored by: Dr. Ruchita Singh

INTRODUCTION
Hantaviruses are globally distributed zoonotic pathogens transmitted to humans primarily through inhalation of aerosolized excreta (urine, droppings, or saliva) from infected rodents, causing severe illnesses like Hantavirus Pulmonary Syndrome (HPS) also known as Hantavirus Cardiopulmonary Syndrome (HCPS) in the Americas and Hemorrhagic Fever with Renal Syndrome (HFRS) in Eurasia. Hantaviruses are a group of viruses that belong to the family Hantaviridae. These viruses are enveloped and possess a tripartite single-stranded negative-sense RNA genome enclosed within a spherical capsid. The disease manifestation and severity can vary depending on the viral strain and geographical region 2,3,4 with symptoms appearing as early as one week or as late as eight weeks following exposure.
In India, the Thottapalayam virus was the first hantavirus identified; however, it has not been clearly associated with significant human disease.
Figure 1: Transmission Pathway
Infected Rodent Reservoir host; sheds virus in urine, droppings and saliva | ➡ | Aerosolisation Rodent excreta dry out and virus-containing particles become airborne in enclosed spaces | ➡ | Human Infection The Primary Route of human infection is Inhalation; transmission may also occur, via direct contact with contaminated materials, or rodent bite/scratch Infection follows exposure. Limited person-to-person transmission is reported with Andes virus |
| ⚠️ High-risk activities: Activities involving close contact with rodents or their habitats, such as cleaning sheds, trapping, farming, or forestry work increase the risk of infection |
DISEASE BURDEN
Hantavirus infection is considered rare in India, with only sporadic human cases reported rather than widespread outbreaks. Only a handful of humans have tested positive, primarily in South India. Studies have identified low levels of hantavirus seropositivity in certain populations, with some reports indicating seroprevalence rates of approximately 4%. However, large-scale outbreaks have not been documented in the country.
China and the Republic of Korea have historically reported thousands of hantavirus infections cases each year, although several regions have observed a gradual decline in case numbers over recent years. The same incidence is observed in Europe; infections are becoming fewer. They are mainly attributed to the Puumala virus in central and northern Europe 1
In Asia and Europe, most hantavirus infections present as Haemorrhagic Fever with Renal Syndrome (HFRS). Disease severity can range from mild to severe, with reported mortality rates generally ranging between 1% - 12%, depending on the viral strain and geographic region. Infections are more commonly reported in rural settings a nd among individuals with occupational or environmental exposure to rodents, particularly males aged 20–40 years3.
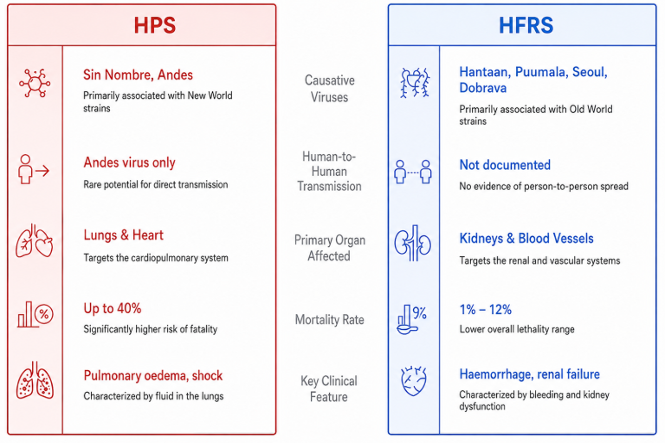
Figure 2: Hantavirus disease in humans
CLINICAL PRESENTATION
Depending upon the type of virus, symptoms usually begin between 1-8 weeks after exposure and may include fever, headache, muscle aches, abdominal pain and nausea or vomiting.
Hantavirus Pulmonary Syndrome (HPS): The HPS typically progresses through four clinical phases3 :
01 Prodrome Fever, headache, muscle aches, nausea. Lasts 3–6 days. | 02 Cardiopulmonary Rapid pulmonary oedema & shock. This is the most critical phase and carries highest mortality risk. | 03 Diuresis Pulmonary oedema clears; fever and shock resolve. | 04 Convalescence Patient recovers. Full recovery may take weeks to months. |
Haemorrhagic Fever with Renal Syndrome (HFRS): The HFRS is characterized by fever, headache, abdominal pain, nausea and haemorrhagic manifestations. Severe cases may progress to hypotension and acute kidney failure 1 .
The severity of the disease varies depending on the virus causing the infection. Hantaan and Dobrava virus infections are generally associated with more severe disease with reported fatality rates ranging from 5-15%. In contrast, Seoul, Saaremaa, and Puumala virus infections are usually more moderate with fatality rates generally below 1% . Complete recovery can take several weeks to months6.
DIAGNOSIS OF HANTAVIRUS INFECTION
Early diagnosis of hantavirus cases can be challenging because the initial symptoms are often non-specific and resemble other febrile or respiratory illnesses.
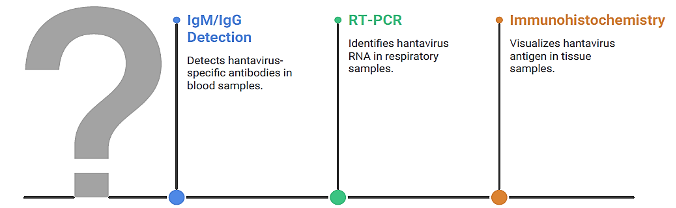
Figure 3: Hantavirus diagnostic markers
TREATMENT
At present there is no specific antiviral treatment available or there is no vaccine for prevention of hantavirus infection. Supportive management, including treatment of respiratory, cardiac, and renal complications, can significantly improve clinical outcomes when initiated early .
Prevention of hantavirus outbreaks depends largely on reducing contact between human and infected rodents, which can be achieved by:
🚫 Avoid exposure to rodents & their droppings | 🏠 Keep homes and work places rodent-free | 🧴 Disinfect contaminated areas |
🔩 Seal rodent entry points in buildings | 💨 Ventilate enclosed spaces before entering | 😷 Use personal protective equipment (PPE) in high-risk areas |
THE 2026 MV HONDIUS (ANDES STRAIN) OUTBREAK
Andes Virus · Cruise Ship–Associated Outbreak Reported by WHO · May 2026 · Multi-country passengers | GLOBAL RISK STATUS LOW | ||
11 CONFIRMED CASES | 3 DEATHS | 0 US CASES REPORTED | 0 INDIA CASES REPORTED |
■ First confirmed shipboard Andes virus transmission — historically, outbreaks were associated with rural or wilderness exposure. ■ WHO, CDC, and ECDC coordinated international response under IHR; all passengers treated as high-risk contacts with quarantine, symptom monitoring, and restricted group activities. ■ Two Indian crew members onboard — both asymptomatic and safe; Indian public health risk assessed as LOW by WHO and Indian health officials. ■ Key uncertainty: single zoonotic introduction with onboard spread vs. multiple parallel zoonotic exposures during shore excursions in endemic regions. ■ Unlike COVID-19 outbreak, Hantavirus infection is generally not airborne; human-to-human transmission of hantavirus is extremely rare (even with Andes strain it requires extremely close and prolonged physical contact and a global pandemic situation is not expected. ■ This low-incidence, high-complexity pattern parallels early Nipah and Ebola events, highlighting preparedness gaps for rare, high-consequence pathogens. | |||
| ⚠️ Case counts are subject to revision. While investigations are ongoing, current evidence suggests a low likelihood of the outbreak progressing into a widespread pandemic, particularly given the limited and inefficient human-to-human transmission observed to date7. |
References:
World Health Organization . Disease Outbreak News: Hantavirus cluster linked to cruise ship travel, Multicounty; 13May2026.
World Health Organization . Hantavirus; 06May2026
Centers for Disease Control and Prevention. About Hantavirus; 13May2024.
Centers for Disease Control and Prevention . Clinical Overview of Hantavirus; 08May2026.
National Collaboration Centre for Infectious Disease. Hantavirus.
World Health Organization . Message by the WHO Director-General to the people of Tenerife regarding the hantavirus response; 09May2026
European Centre for Disease Prevention and Control . Questions and answers on the hantavirus outbreak in a cruise ship; 14May2026.